Secondary
- Ordinary curriculum including project and self-made textbook
- Digestion - physical and/or chemical breakdown of food
- Physical digestion: mechanical rending to increase surface area for chemical digestion
- cheese trimmer
- mouth - teeth to chew, masticate
- stomach - rugal folds to churn - chyme
- HCl actually break down the cconnective tissue, but not into the amino acids
- liver - bile emulsified lipids, still triglyceride
- Chemical digestion: breaking down the large molecules (polymers) into smaller soluble molecules (monomers) for easy absorption primarily via hydrolysis
- lipid + water - (lipase) glycerol + fatty acids or monoglyceride + fatty acids
- lipase is catalyzing the water digesting lipid, not the digesting agent
- foods - polymers, macromolecules
- into small molecules, like glycogen to glucose
- Pathways: into the breach
- Mouth
- Teeth
- physical digestion: omnivore (all to eat) with large brains of bigger memory storage; our ancestors gatherer hunter; gorilla (vegetarian), chimpanzee (omni)
- carnivore (meat to eat) = incisors (chisel-shaped teeth for biting or cutting), canine (hold, tear)
- How many canines does a person have? - 8 including baby teeth and adult); wearing down the canine is common in the ancient
- herbivore (plant to eat) = premolars and molars (both grind); successful way to survive
- Saliva - mostly water and mucus with mucin (glycoprotein), as lubricant
- Salivary glands - pH 7
- salivary amylase optical pH 6.7-6.9, temperature will be 32-37 celcius
- rich in salivary amylase converting Amylose to maltose
- starch = amylopectin + amylose (10%)
- Amylose + water - (amylase) maltose
- clear mineralization
- Bolus - masticated food ball
- sensors on tongue: sweet, sour, bitter, umami (trigger savary, meat, MSG), salty
- Swallowing steps - Deglutition (to draw on your own)
- Bolus presses on the pharynx stimulate a swallowing (gulp, involuntary by autonomic nervous system) response
- touch pharynx (back of the throat) of a dog/cat, they would throw up
- Larynx - voice box
- Palate seals off the nasal cavity, preventing food from entering
- don't talk with your mouth full
- Stops breathing and the epiglottis seals off the trachea
- the esophageal sphincter relaxes, food goes down to the alimentary canal
- Esophagus (food pipe)
- upper esophageal muscle
- no digestion
- Peristalsis - wave-like, rhythmical contractions of circular smooth involuntary muscles (ANS)
- Stomach
- pH: actively digesting 1-3, resting 4-5
- Cardiac sphincter - champagne cord, limit the back flow of gastric juices
- failure - acid reflux or heartburn
- Pyloric sphincter - (gate keeper)
- limit the flow of gastric juices (pH 1-3) into the small intestine (pH 6-6.5, duodenum), which normally denature the intestinal juices critical for digestion
- Rugae - allow for expansion of the stomach after food consumption; rugal folds to churn the chyme
- Gastric pits - cardia, fundus, pylorus; source of the stomach's digestive juices - pH 1-3
- Parietal cells - secretes concentrated HCl
- HCl - breaking up connective tissue to increase ; killing surface bacteria, reacting with pepsinogen
- Pepsinogen - made in chief cells; Pepsinogen (protein) + HCl - Pepsin (enzyme, in turn activate more pepsinogen)
- Chief cells - secrete pepsinogen, (pepsin precursor), in stomach, reacting with HCl to produce pepsin
- protein + water - (pepsin as enzyme) amino acid strands (polypeptide/peptide fragments, clast = fragments)
- Brad's Drink - pepsi (kola nuts)
- Surface mucous cell - Mucus (mucin) secreted = bicarb layer (buffer), also site of pepsin
- protect stomach lining from autodigestion and abrasion, or lubricant for food passage
- failure - ulcer
- causes:
- bacterial (helicobacter pylori) infection
- treatment: antibiotic regime
- excessive use of NSAIDS (non steroid anti inflammatory drug), e.g. aspirin, ibuprofen, naproxen
- Gastric ulcer - stomach; peptic ulcer- digestive tract
- mucus also in salivary glands, esophagus, small intestine, colon, respiratory tract (bronchi, nose), reproductive tract (cervix - pattern of reproduction, cowper's gland)
- Brunner's gland at Duodenum - alkaline mucus to neutralize acid chyme from the stomach
- Chyme - semi-fluid, partially digested mass exiting the stomach
- pH 2, stained by bile giving a green or brown colorish
- pablum - flavorless, instant food supplement
- Chimera - single organism made of cells from two individuals
- Small intestine - 3 part (American English tend to drop the e)
- Duodenum - (duo2+de10+num-figure) - twelve fingers; site of digestion, producing and receiving numerous digestive enzymes and hormones and bile, related with liver and pancreas
- imperial inch - width of king's finger; Napoleon 5'4 - 5'7
- 30 cm, pH 6-6.5
- Jejunum & ileum - tube about size of hot dog weiner (0.5m^2, 150-200m^2) - sausage, with ~ 6m (if stretched), with pH 7-8, site of absorption (90% of the nutritions, e.g. vitamins are not necessarily absorbeddue to solubility), loaded with capillaries
- folds, villi
- Villi - with capillaries taking up glucose and amino acids; also lacteals taking up glycerol and fatty acids
- where's blood, there's lymph (milk-color)
- Microvilli - of brush border cels, finger-like projections, also found in the kidneys (PCT, proximal tubule)
- Carbohydrates absorption
- taken up as monosaccharides e.g. glucose, via capillaries - hepatic portal vein - liver; excess glucose stored as glycogen by insulin; released as needed to maintain homeostasis (4-5.5 mmol/L) by glucagon
- extra excessive converted to lipid (irreversible) causing fatty liver
- cellular uptake is via both **active transport in ** small intestine and kidney ; also facilitated transport at most other cells (tend to be poor in glucose)
- active transport driven by a Na+ gradient; co-transport of 2 Na+ and 1 glucose, moving against the concentration gradient; e.g. salt on chocolate, body seeing it as sweeter
- sports medicine and endurance training
- insulin binds with receptor - calls up secretory vesicles with GLUT proteins - exocytosis to the membrane - glucose enters cell via facilitated transport
- Diabetes: type I no insulin, type II insulin resistant
- a diet high in processed carbohydrates, with glycemic index (GI) > 70 = high sugar (sucrose) or fructose direct can increase the risk of type II diabetes (insulin resistance), heart disease (excess glycogen forms triglycerides), cancer, and metabolic syndrome
- Metabolic syndrome (exercise lower risks not physical appearance)
- marked by abdominal obesity, blood fat disorders (atherogenic dyslipidemia), elevated blood pressure, insulin resistance, prothrombotic state, proinflammatory state
- Protein absorption
- absorbed as amino acids via capillaries - hepatic portal vein - liver - plasma proteins in blood
- e.g. albumin (buffer, osmoregulator), prothrombin (blood clotting agent), fibrinogen
- Deamination - of proteins; amino acid - amino group - ammonia NH3 (v. toxic in dose) - converted by the liver to urea (less toxic) for excretion via the kidneys
- NH3 + CO2 - urea
- Buffer: NH3 + H+ - NH4+ (ammonium ion)
- in the US, meat dominant meals - colorectal caner risks surge
- Lipids absorption
- absorded as initially glycerol (monoglyceride) and free fatty acids, via lacteals (lymph) - to the body - subclavian vein - superior vena cava - heart
- digestion in the duodenum, fat - fat droplets by bile; and** lipase from pancreas**, turned to simple fats (glycerol fatty acid) at small intestine villi both physical and chemical; at small intestine simple fats back to triglyceride
- taken up by villi cells: simple fats resembled to triglycerides - chylomicron (lipoprotein = proteins + phospholipids + cholesterol coating) - lacteals, lymph vessels
- muscle and adipose tissues taking up the triglycerides for storge and energy use
- & back to the liver for cholesterol synthesis (VLDL - (if extra) LDL, HDL) and lipid synthesis (e.g. triglyceride)
- VLDL - very low density lipoprotein, delivering fat and cholestrol to body, once done, it returns to the liver and remainder gets made to LDL
- Low-density Lipoprotein (LDL) delivers fat and cholesterol to body before returning to the liver
- High-Density Lipoprotein (HDL) travels around the body picking up excess cholesterol; source: liver and small intestine
- Hyperbilirubinemia - too much Bilirubin in blood
- mid-east people genetically prone to have high-cholesterol
- Large intestine (colon, bowels)
- cecum (cec- for container), appendix (vestigial), ascending, transverse, descending, sigmoid (like a sigma, S-shaped), rectum, anus
- ~1.5m, pH 7-5.5 (acidic)
- Water reabsorption: 7-10 L/day, #1 site
- excretion of excess: iron salts (Na) and Ca salts
- site of bacteria etc.
- E.coli - generally mutualistic (beneficial) symbiont
- that inhibits colonization by harmful bacteria
- synthesizes Vitamin esp vitamin K, and B (e.g. folic acid)
- produce amino acids and other growth factors
- SIBO - small intestinal bacterial overgrowth; abnormal increase in the overall bacterial population in small intestine
- functions to compact the undigested wastes left over from digestion for easier elimination / defecation
- feces - 60% dry bacteria, 40% undigested dead cells
- compaction (alzheimer constipation)
- appendix truly important in cows; also part of the lymph tissue (also like tonsil), store backup bacteria
- deterostome: first anus, second mouth; - stome (opening); e.g. echinoderms like seastar; human
- protostomes: mouth first; most others
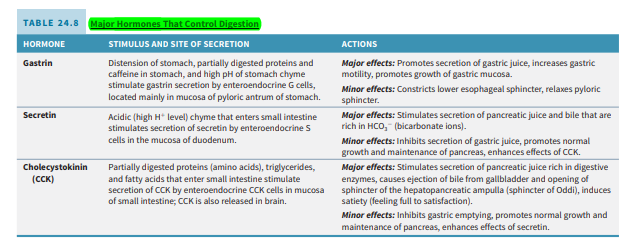
- Hormones
- Gastrin - stimulated at stomach when bolus passes through the cardiac sphincter
- stimulate HCl production and increases stomach motility (churning)
- Secretin - produced at duodenum, stimulated by acid-rich chyme (in presence of HCl)
- stimulate the release of sodium bicarbonate from pancreas
- buffer acid chyme from pH 2 - pH -7
- stimulate release of alkaline bile from gall bladder
- CCK - Cholecystokinin, bile sac movement
- produced at duodenum - upper small intestine
- for lipid-rich and protein-rich chyme
- stimulate gall bladder to release bile as emulsifier
- stimulate pancreas to release digestive enzymes (lipase)
- CCK & Secretin - together inhibit peristalsis and HCl production - slow digestion
- Bile - emulsification
- sourced at liver
- stored in the gall bladder
- a surfactant, increases SA for enzyme lipase activity
- cancer cells - gluttons biomagnification for chemotherapy drugs
- Parasympathetic stimulation - rest and digest; decrease heart rate, slow and deep breath; activate stomach and intestinal glands, motibility of the wall
- for human: it's the normal state
- Sympathetic stimulation - fight or flight; increase heart rate, fast and shallow breathing rate; inhibit stomach and intestinal glands, no motility of the wall
- for bear: sympathetic is normal
- Insulin & glucagon - antagonistic hormones
- Insulin lowers blood glucose, convert and stores glucose as glycogen at liver mostly and also muscle, reaching homeostatic 4-6 mmol/L
- Glucogenesis - or gluconeogenesis, in the liver and kidney helps to maintain the glucose level in the blood - brain and muscle can extract sufficient glucose from it to meet their metabolic demands.
- if blood glucose is high, negative feedback until blood glucose low at normal
- Edmonton protocal: a method of implantation of pancreatic islets for the treatment of type 1 diabetes mellitus, specifically "brittle" type 1 diabetics prone to hypoglycemic unawareness.
- Glucagon raises blood glucose, converting stored glycogen to glucose
- Liver - 6 functions
- Bile synthesis - surfactant, emulsifier of lipids, alkaline (pH 7.5-8.8), neutralize gastric acids in the small intestine
- Excretion of bilirubin; biliverdin (breaking down red blood cells) - metabolite (metabolic waste product)
- Gilbert Syndrome - a mild genetic disorder in which the liver does not properly process the bilirubin
- Protein & lipid synthesis:
- plasma proteins; rich in rough ER for albumin, prothrombin, fibrinogen
- lipid synthesis in smooth ER, like cholesterols (HDL, LDL), triglycerides etc
- Glucose homeostasis
- Glycogenesis - glucose - glycogen (insulin)
- Gluconeogenesis - glycogen - glucose (glucagon)
- site of insulin breakdown
- Storage: iron, copper; vitamin A,B,D...; glycogen
- Deamination - breakdown excess proteins and form ammonia - urea
- Detoxification: smooth ER
- converting ammonia to urea for excretion
- breaking down insulin and other hormones
- breaking down hemoglobin to bilirubin into bile
- general detoxification of toxic substances;
- eat with caution
- Enzymes (simplified)
- salivary glands (pH-7): salivary amylase - amylose to maltose
- stomach (pH 1-3): pepsin (protease) - protein to amino acids strands (peptide fragments)
- duodenum (optimal pH~8): operates within small intestine
- peptidase - aid in breaking down peptides to amino acids
- nuclease - nucleic acids to nucleotides
- maltase - maltose to glucose
- sucrase - sucrose to glucose + fructose
- lactase - lactose to glucose + galactose
- pancreas (optimal pH ~8):
- pancreatic amylase - amylose - maltose
- trypsin (protease) - trypsinogen in pancreas and become trypsin as entering small intestine - protein - amino acids
- nuclease - nucleic acids - nucleotides
- lipase - lipids - glycerol & fatty acids
- Nutrition vs enzyme
- polysaccharides (amylose) - salivary amylase (pH7), pancreatic amylase (pH 8+, in small intestine) - maltase (small intestine) - glucose
- proteins - pepsin (stomach pH 1-3), trypsin (sourced at pancreas and functions in small intestine - pH 8) - peptides - peptidase (small intestine) - amino acids
- lipids - bile from liver emulsify increasing SA, pancrease lipase - glycerol (monoglycerides) fatty acids
- nucleid acids - pancreas nuclease and intestinal nuclease - nucleotide - nucleotidase - nucleosides + phosphate - nucleosidase - sugar + base
- Label
- Larynx (L-front), Pharynx (P-back)
- avoid eating before going to bed, no lipid preferably
- Hepatic portal vein - into the liver; rich in amino acids and glucose, poor in lipids
- Hepatic vein - poor glucose, rich proteins, lipids - out
- Liver out inferior vena cava
- Lab
- a paragraph of reflection
- adds on; up to me; completing a table of what we take in and nutritional label
- extra
- women entering early menopause at the risk of diabetes
- painkiller should be selected specifically for a patient; seniors can't metabolize the coating of painkillers
- Interesting stuff
- secrete: release for reason, e.g. hormone; excrete: release of metabolic waste
- digestive: secrete bile - lipid; HCl secreted
- circ: bile excrete
- small intestine - disaccharidases - nuclease - peptidase
- calaries load -1500 or so
- product - vitamin water - leave the fat table
- Test
- accessory digestive organs: liver, pancreas
- check -ase vs -ose
Kaplan
MeSH
- Biliary Tract [A03.159]
- Gastrointestinal Tract [A03.556]
- Liver [A03.620]
- Pancreas [A03.734]
BIOL235
- 24.1 Overview of the digestive system, p. 831
- identify the organs of the digestive system.
- describe the basic processes performed by the digestive system.
- 24.2 Layers of the GI tract. p. 832
- describe the structure and function of the layers that form the wall of the gastrointestinal tract.
- Mucosa
- Submucosa
- Muscularis
- Serosa
- 24.3 Neural innervation of the GI tract, p. 834
- describe the nerve supply of the GI tract.
- Enteric nervous system
- Autonomic nervous system
- Gastrointestinal reflex pathways
- 24.4 Peritoneum, p. 835
- describe the peritoneum and its folds.
- 24.5 Mouth, p. 837
- identify the locations of the salivary glands and describe the functions of their secretions.
- describe the structure and functions of the tongue.
- identify the parts of a typical tooth and compare deciduous and permanent dentitions.
- Teeth
- Mechanical and chemical digestion in the mouth
- 24.6 Pharynx, p. 843
- describe the location and digestive function of the pharynx.
- 24.7 Esophagus, p. 844
- describe the location, anatomy, histology, and functions of the esophagus.
- Histology of the esophagus
- Physiology of the esophagus
- 24.8 Deglutition, p. 845
- describe the 3 phases of deglutition.
- 24.9 Stomach, p. 846
- describe the location, anatomy, histology, and functions of the stomach.
- Anatomy of the stomach
- Histology of the stomach
- Mechanical and chemical digestion in the stomach
- 24.10 Pancreas, p. 852
- describe the location, anatomy, histology, and function of the pancreas.
- Anatomy of the pancreas
- Histology of the pancreas
- Composition and functions of pancreatic juice
- 24.11 Liver and gallbladder, p. 854
- describe the location, anatomy, histology, and functions of the liver and gallbladder.
- Anatomy of the liver and gallbladder
- Histology of the liver and gallbladder
- Blood supply of the liver
- Functions of the liver and gallbladder
- 24.12 Small intestine, p. 859
- describe the location and structure of the small intestine.
- Anatomy of the small intestine
- Histology of the small intestine
- identify the functions of the small intestine.
- Mechanical digestion in the small intestine
- Chemical digestion in the small intestine
- Absorption in the small intestine
- Role of intestinal juice and brush-border enzymes
- 24.13 Large intestine, p. 869
- describe the anatomy, histology, and functions of the large intestine.
- Anatomy of the large intestine
- Histology of the large intestine
- Mechanical digestion in the large intestine
- Chemical digestion in the large intestine
- Absorption and feces formation in the large intestine
- The defecation reflex
- 24.14 Phases of digestion, p. 875
- describe the 3 phases of digestion.
- Cephalic phase
- Gastric phase
- Intestinal phase
- Major hormones that control digestion
- describe the major hormones regulating digestive activities. @@
Other hormones of the digestive system